What is the cranial cruciate ligament?
The cranial cruciate ligament (CrCL) in dogs is the same as the “anterior” cruciate ligament (ACL) in humans. It is a band of tough fibrous tissue that attaches the femur (thigh bone) to the tibia (shin bone), preventing the tibia from shifting forward relative to the femur. It also helps to prevent the stifle (knee) joint from over-extending or rotating.
band of tough fibrous tissue that attaches the femur (thigh bone) to the tibia (shin bone), preventing the tibia from shifting forward relative to the femur. It also helps to prevent the stifle (knee) joint from over-extending or rotating.
Trauma to the equivalent ligament in humans is common, and damage most frequently occurs during some form of sporting activity (including football, rugby, and golf). The nature of cranial cruciate ligament disease is very different in dogs. Rather than the ligament suddenly breaking due to excessive trauma, it usually degenerates slowly over time, rather like a fraying rope. This important difference is the primary reason why the treatment options recommended for cruciate ligament injury in dogs are so different from the treatment options recommended for humans.
What is the cause of cruciate ligament injury in dogs?
In the vast majority of dogs, the cranial cruciate ligament (CrCL) ruptures as a result of long-term degeneration, whereby the fibers within the ligament weaken over time. We do not know the precise cause of this, but genetic factors are probably most important, with certain breeds being predisposed (including Labradors, Rottweilers, Boxers, West Highland White Terriers, and Newfoundlands). Supporting evidence for a genetic cause was primarily obtained by assessment of family lines, coupled with the knowledge that many animals will rupture the CrCL in both knees, often relatively early in life. Other factors such as obesity, individual conformation, hormonal imbalance, and certain inflammatory conditions of the joint may also play a role.
How can I tell if my dog has cruciate ligament disease?
Limping is the commonest sign of CrCL injury. This may appear suddenly during or after exercise in some dogs, or it may be progressive and intermittent in others. Some dogs are simultaneously affected in both knees, and these dogs often find it difficult to rise from a prone position and have a very “pottery” gait. In severe cases, dogs cannot get up at all and can be erroneously suspected of having a neurological problem.

What is happening inside an affected joint after cruciate ligament injury?
Fraying of the ligament triggers a cascade of events resulting in knee pain and lameness. At the earliest stage, osteoarthritis is already present. It’s important to accept this, because many people ask “when will my dog get osteoarthritis?” when in fact the dog has it already. At a critical point of fraying, the CrCL loses its normal mechanical function and painful lameness is accompanied by a mechanical lameness. At this point, one of the factors influencing the mechanical lameness is the shape of the top of the tibia (shin bone) which has a pronounced backwards slope in dogs. The consequence of this slope in dogs with an incompetent CrCL is that the femur will roll down the slope every time weight is taken on the leg. In dogs without impairment of the CrCL, this slope will only become a problem if it is very steep indeed and can predispose to CrCL problems.
In some dogs, the mechanical deficiency can result in trauma to other structures within the joint, in particular, a pair of buffer cartilages known as menisci. In slipping down the slope of the top of the tibia, the femur can crush and tear these cartilages, particularly the one on the inside (medial aspect) of the joint.
How is cranial cruciate ligament injury diagnosed?
Diagnosis in dogs with complete rupture of the CrCL is usually based on examination by an experienced orthopedic surgeon, with a demonstration of laxity of the joint by specific manipulations of the knee. In dogs with partial tears or early degeneration of the ligament, other tests may be necessary, including radiography (x-rays) or MRI scans. To be of maximum benefit, radiographs must be of optimal quality. In most dogs, exploratory surgery or arthroscopy (keyhole surgery) is used to confirm the diagnosis and to investigate for possible cartilage tears or other problems.
How is cruciate ligament injury treated?
Non-surgical management
Non-surgical management is seldom recommended, except where the risks of a general anesthetic or surgery are considered excessive (e.g. patients with severe heart disease, uncontrolled hormonal disorders or immune conditions, etc.). The cornerstones of non-surgical treatment are bodyweight management, physiotherapy, exercise modification, and medication (anti-inflammatory painkillers). These same techniques are also important in the short-term management of dogs who are treated surgically, although the primary surgical aim is to minimize the requirement for long-term exercise restriction and medication. Dogs greater than 15kg have a very poor chance of becoming clinically normal with non-surgical treatment. Dogs weighing less than 15kg and cats have a better chance, although improvement usually takes several months and is rarely complete. At Oakdale Veterinary Group we are able to provide you and your dog with a rehabilitation plan for cruciate ligament disease.
Surgical management
Surgical treatments are categorized into techniques that aim to replace the deficient ligament and those that render the ligament redundant by cutting the tibia and re-aligning the forces acting on the stifle joint.
Ligament replacement techniques
Various surgical techniques that mimic the procedures used for ligament replacement in humans have been practiced for more than five centuries. In dogs, techniques using the transfer of local tissues have the poorest chance of returning limb function to nearly normal or normal. This is probably because the replacement tissues are not as robust as the original ligament and they are positioned in the same unfavorable biomechanical environment that caused the original ligament to fail in the first instance.
Prosthetic ligament replacement techniques have also been used for many years. These are simple techniques that have the ability to return many animals to nearly normal function. The primary disadvantages of these techniques are their unpredictability during the early stages of recovery and mechanical limitations in heavy and athletic dogs. Some dogs become transiently ‘more lame’ before improvement occurs. Others take many weeks to improve and a proportion will have ongoing knee instability and pain. Variations of this technique are most commonly recommended for dogs with traumatic cruciate ligament injuries and in animals where several stabilizers of the knee are damaged, so-called “multi-ligamentous injuries”.
For decades, sutures of nylon with various knotting and crimping systems have been placed between a bone at the back of the femur (the fabella) and a tunnel in the top of the tibia. These so-called fabello-tibial tuberosity sutures have had variable reported success rates dependent on material and technique. The most important aspect of this technique is that the ligament origin on the femur and insertion on the tibia are as isometric as possible, i.e. stay as far as possible the same length in flexion and extension. In reality, this is impossible and so the principle has been referred to as “quasi-isometry”. High success rates have been reported for the Arthrex “TightRope™” technique which uses a synthetic material called Fibretape™ or Fibrewire™ on metallic anchors placed through bone tunnels in the femur and the tibia. In patients where we adopt ligamentous replacement, this is the commonest technique we employ for this purpose.
Treatments that render the cranial cruciate ligament redundant
These surgeries alter the geometry of the affected knee joint in such a way that the CrCL is no longer necessary to maintain stability. There are several variations in the technique, with all involving reshaping of the top of the shin (tibia) by cutting of the bone and fixing it in a new position.
Tibial Plateau Leveling Osteotomy (TPLO)
This surgery involves creation of a radial cut in the top of the tibia and rotation of the plateau segment until the previous slope in the bone is no longer present. The bone is subsequently fixed in this new position using a bone plate and screws.
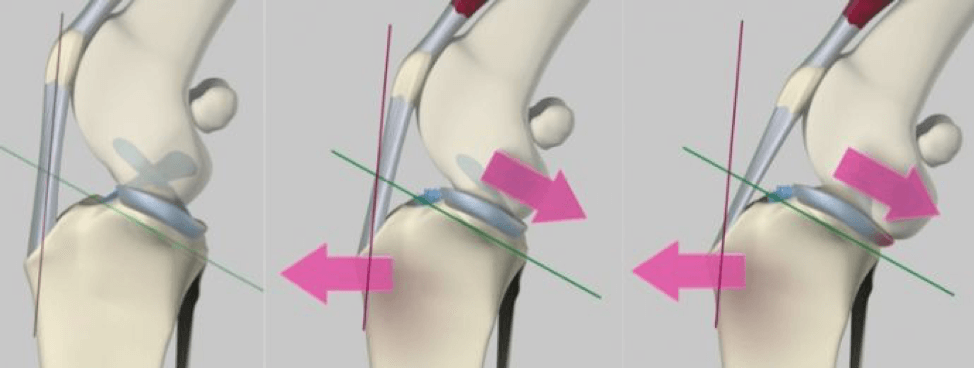
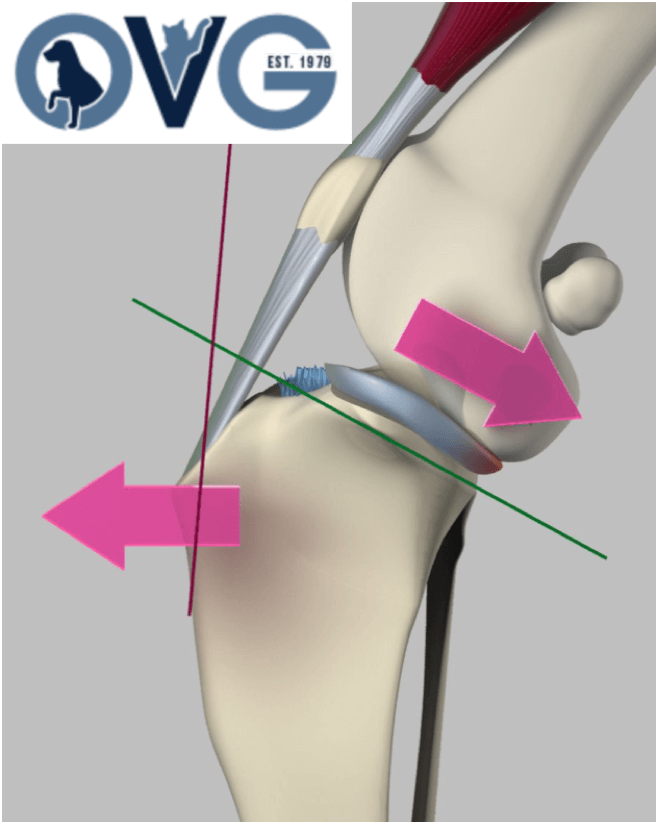
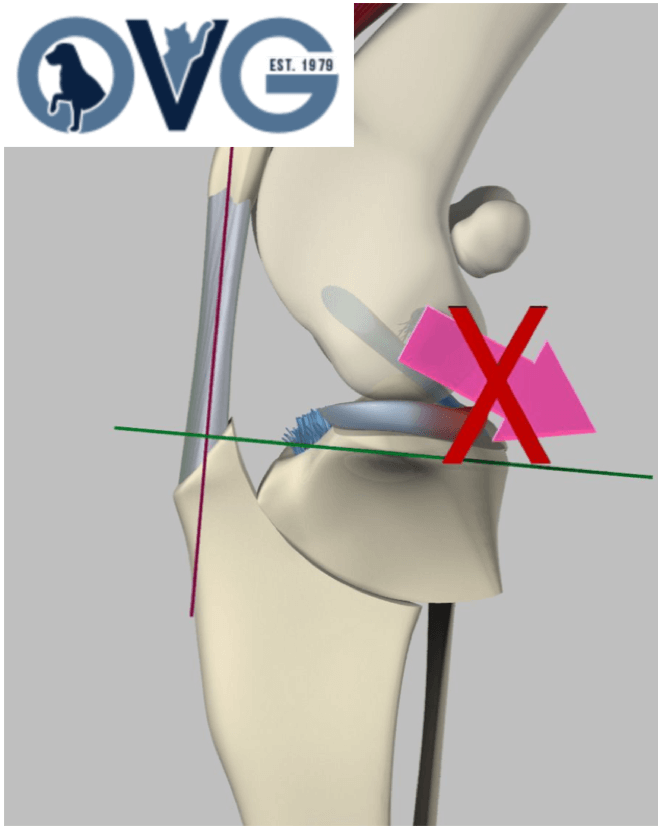
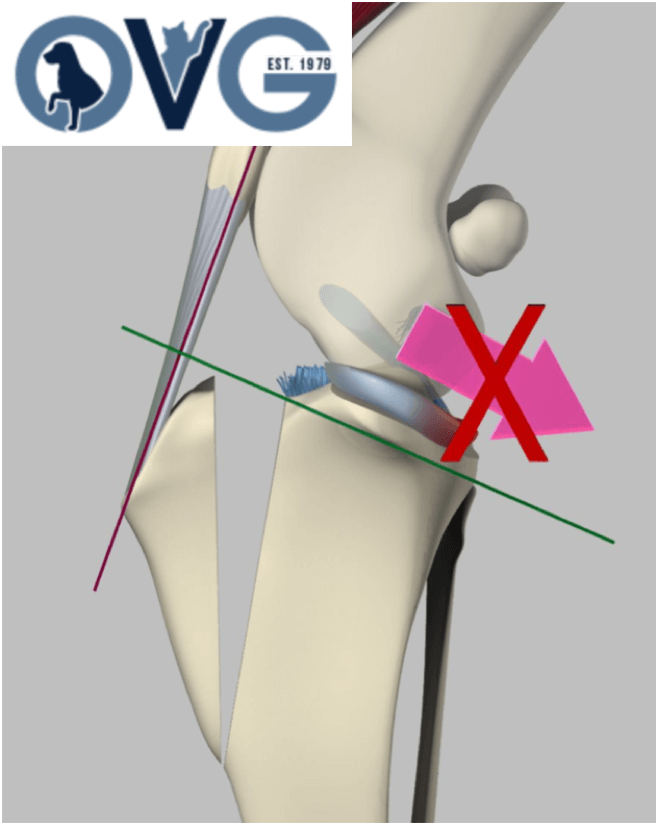
Tibial Tuberosity Advancement (TTA)
This surgery follows the same principle as TPLO, with a cut being created in the tibia to allow a change in geometry that renders the CrCL redundant. The mathematical principles behind TTA are more complex than those behind TPLO; however, the basic principle is that an altered direction of traction from the quadriceps muscle group produces a force across the knee joint that neutralizes the tendency for the femur to roll down the slope of the tibial plateau. In effect, both TTA and TPLO aim to render the tibial plateau perpendicular to the straight patellar tendon and in so doing, neutralize the tendency for the femur to slip down the slope of the tibia.
Play
What are the advantages of surgeries like TPLO and TTA that involve cutting of bone?
Because bone healing is more efficient than ligament healing, these repairs have a reputation for being significantly more robust than surgeries designed to replace the damaged ligament. The major practical benefit is a very reliable return of limb use, with all dogs expected to start weight bearing on the operated limb within 1-3 days. The mechanical advantages of TPLO and TTA coupled with the rapid return to function is especially important for heavy dogs, athletic animals, animals presenting with mild lameness (where ligament replacement could make them significantly more lame initially), and in animals with CrCL injuries affecting both stifle joints. In some animals with CrCL injuries that simultaneously affect both knees, TPLO can be performed on both stifles in a single surgery. The decision of whether TPLO or TTA is most appropriate is made based on the anatomy of the individual. In many cases, either surgery would constitute a suitable and appropriate choice.
How is the medial meniscus examined during cruciate ligament surgery?
All dogs have an inspection of the joint to assess whether secondary injuries to the buffer cartilages, known as menisci, have occurred. If an injury is found, this is treated surgically by meniscal trimming.
What are the success rates of TPLO and TTA?
As a general rule, over 90% of dogs return to normal activity after TPLO or TTA. This generally means that dogs are so normal that owners are unable to detect lameness at home. We expect dogs to return to unrestricted exercise without any requirement for ongoing medications. Performance dogs including sniffer dogs and military patrol dogs are expected to return to work after these surgeries. The success rates for TPLO and TTA are very similar.
What are the potential problems or complications after cruciate ligament repair surgery?
Fortunately, complication rates are low when experienced surgeons perform cruciate ligament repair surgery. The two commonest complications are infection and mechanical complications. Infection is treated using antibiotics. In some cases, surgical irrigation is necessary and, in the worst cases where bacteria adhere to the implants, the implants must be removed after the bones have healed. In the vast majority of animals, the implants remain in place for life and cause no problems at all. Mechanical complications usually occur in dogs that exercise too much before the bones have healed (which takes about 6 weeks). Many mechanical complications are managed with rest alone, although some problems require surgical revision. A rare complication of late injury to the menisci (buffer cartilages) within the operated knee joint can require treatment. Other rare complications including sprains and strains around the knee joint can generally be managed using physiotherapy alone.